Is Your Resuscitation Fluid Harming Your Patients?


Dr. Juan M. Galvis
Introduction.
For decades, physicians have discussed which crystalloid fluid is the best fluid for resuscitation and for many years patients were resuscitated with normal saline. This brief article will discuss which crystalloid is the most appropriate for resuscitation based on the most recent evidence.
It is believed that the first crystalloid fluid originated during the Indian blue cholera pandemic in 1831. Later in the 1880s, Dr. Sydney Ringer determined the optimal electrolytic concentrations; sadly, his findings were not adopted until several decades later. At the moment, in 2021, we have several crystalloids that range from average saline 0.9% concentration, Ringer's lactate, Plasmalyte, Normosol, and many more.
The principal of prescribing intravenous fluids in medicine has been practiced since the 19th century cholera pandemic, the world wars, and subsequent 20th century. In the dawn of the 21st, Dr. Rivers et al. reported that patients admitted with septic shock will benefit from early goal-directed therapy which included in one of the elements intravenous IV fluids, this included crystalloids.
The therapy became standard of care after the study showed a decrease mortality of 16%. After this study, the use of crystalloids solidified across the world and subsequently brought to question which crystalloid should be prescribed to patient's in the intensive care unit.
Composition.
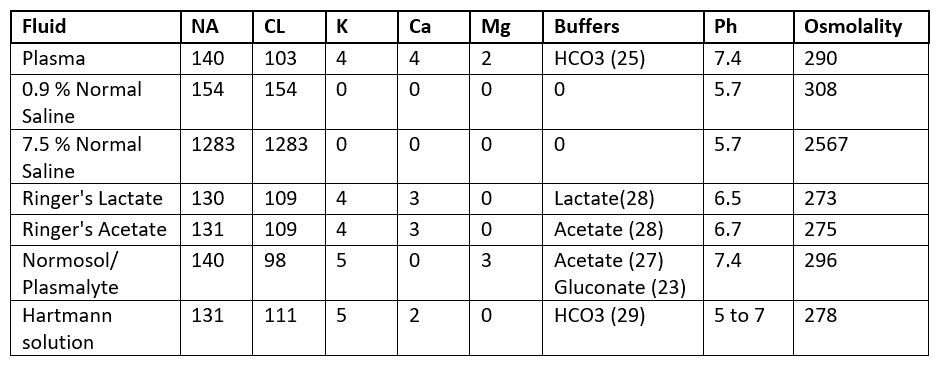
Evidence.
Medical evidence indicates that isotonic crystalloids are not created equal. For the last decade several studies have shown evidence of this. Considering normal saline as a hyperchloremic solution, several studies in animals showed the effects of high chloride causing severe renal vasoconstriction, reduced glomerular filtration rate, and increase of renin activity. The first studies comparing normal saline to Plasma-Lyte came from the surgical literature. Dr. Macfarlane and Lee described higher serum sodium concentration and lower bicarbonate concentration in patients that underwent major abdominal surgery. In 22,851 surgical patients, normal saline was noticed because hyperchloremia was associated with higher 30-day mortality, increased length of stay, and postoperative kidney dysfunction.
In the surgical scientific journals it has been shown that Plasma-Lyte is superior to normal saline in reducing the frequency of hyperchloremia and acid-base disturbances.
In 2018, balance crystalloids versus saline in critical care adults were published in the New England Journal of Medicine. This study concluded among critically ill adults that the use of balanced crystalloids for intravenous fluid administration resulted in a lower rate of the composite outcome of death from any cause, new renal replacement therapy, or persistent renal dysfunction than the use of saline.
This breakthrough is the first step that normal saline should be avoided in the critical ill population.
Why is there resistance to change?
The medical community has been concerned for years of two problems regarding balanced solutions; hyperkalemia and cost.
Hyperkalemia:
Evidence supports that balanced solutions are generally safe with appropriate monitoring. Several studies have shown that balanced solutions do not harm clinical situations such as rhabdomyolysis, diabetic ketoacidosis, and kidney transplant.
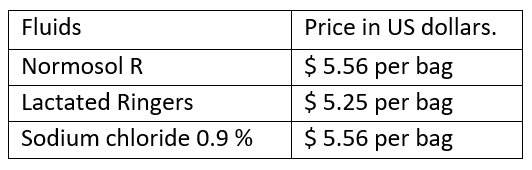
Cost:
The other primary concern is price. Normal saline has been marketed as a cheap crystalloid. The cost of crystalloids in our hospital pharmacy are reflected in the table below, and there is no difference on the price, so the myth of the cost is debunk it.
Conclusion:
In conclusion, the preliminary evidence supports the use of Ringer’s lactate and Plasmalyte over Normal saline in the intensive care population, and new data will come in the upcoming years. Currently, there are several ongoing studies regarding balanced crystalloids in the ICU, such as. The PLUS (Plasmalyte 148 v Saline) and The BaSICS study (Balanced Solution versus Saline in Intensive Care Study) these two extensive multicenter studies that will be light on which fluid should be prescribed to our critical patients.

Juan M. Galvis M.D.
University of Louisville | Assistant Professor of Medicine
Dr. Juan Galvis is an Assistant Professor of Medicine in the Division of Pulmonary Critical Care and Sleep Medicine at the University of Louisville School of Medicine. His clinical expertise is in General Pulmonary and Critical Care Medicine. He completed his residency at the Texas Tech University Health Sciences Center and attended medical school at la Universidad Católica de Santiago de Guayaquil.
References:
Myburgh JA, Mythen MG. Resuscitation fluids. N Engl J Med 2013;369: 1243–1251.
Semler MW, Self WH, Wanderer JP, et al. Balanced crystalloids versus saline in critically ill adults. N Engl J Med. 2018;378:829-839.
Rivers E,Nguyen B, Havstad S, et al.: Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med.
JB Young, GH Utter, CR Schermer, et al.: Saline versus Plasma-Lyte A in initial resuscitation of trauma patients: a randomized trial. Ann Surg.
N Hadimioglu, I Saadawy, T Saglam, et al.: The effect of different crystalloid solutions on acid-base balance and early kidney function after kidney transplantation. Anesth Analg.
